 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeRe-defining Radiology Quality Assurance (QA) -- Artificial Intelligence (AI)-Based QA by Restricted Investigation of Unequal Scores (AQUARIUS)
May 03, 2022There is an urgent need for streamlining radiology Quality Assurance (QA) programs to make them better and faster. Here, we present a novel approach, Artificial Intelligence (AI)-Based QUality Assurance by Restricted Investigation of Unequal Scores (AQUARIUS), for re-defining radiology QA, which reduces human effort by up to several orders of magnitude over existing approaches. AQUARIUS typically includes automatic comparison of AI-based image analysis with natural language processing (NLP) on radiology reports. Only the usually small subset of cases with discordant reads is subsequently reviewed by human experts. To demonstrate the clinical applicability of AQUARIUS, we performed a clinical QA study on Intracranial Hemorrhage (ICH) detection in 1936 head CT scans from a large academic hospital. Immediately following image acquisition, scans were automatically analyzed for ICH using a commercially available software (Aidoc, Tel Aviv, Israel). Cases rated positive for ICH by AI (ICH-AI+) were automatically flagged in radiologists' reading worklists, where flagging was randomly switched off with probability 50%. Using AQUARIUS with NLP on final radiology reports and targeted expert neuroradiology review of only 29 discordantly classified cases reduced the human QA effort by 98.5%, where we found a total of six non-reported true ICH+ cases, with radiologists' missed ICH detection rates of 0.52% and 2.5% for flagged and non-flagged cases, respectively. We conclude that AQUARIUS, by combining AI-based image analysis with NLP-based pre-selection of cases for targeted human expert review, can efficiently identify missed findings in radiology studies and significantly expedite radiology QA programs in a hybrid human-machine interoperability approach.
Tracking Results and Utilization of Artificial Intelligence (tru-AI) in Radiology: Early-Stage COVID-19 Pandemic Observations
Oct 14, 2020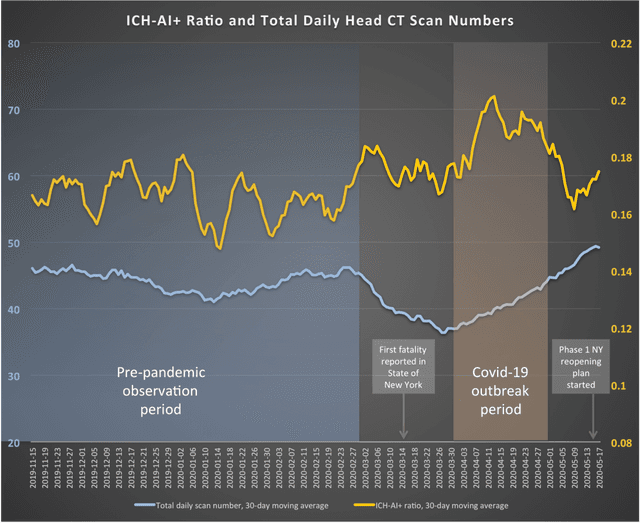

Objective: To introduce a method for tracking results and utilization of Artificial Intelligence (tru-AI) in radiology. By tracking both large-scale utilization and AI results data, the tru-AI approach is designed to calculate surrogates for measuring important disease-related observational quantities over time, such as the prevalence of intracranial hemorrhage during the COVID-19 pandemic outbreak. Methods: To quantitatively investigate the clinical applicability of the tru-AI approach, we analyzed service requests for automatically identifying intracranial hemorrhage (ICH) on head CT using a commercial AI solution. This software is typically used for AI-based prioritization of radiologists' reading lists for reducing turnaround times in patients with emergent clinical findings, such as ICH or pulmonary embolism.We analyzed data of N=9,421 emergency-setting non-contrast head CT studies at a major US healthcare system acquired from November 1, 2019 through June 2, 2020, and compared two observation periods, namely (i) a pre-pandemic epoch from November 1, 2019 through February 29, 2020, and (ii) a period during the COVID-19 pandemic outbreak, April 1-30, 2020. Results: Although daily CT scan counts were significantly lower during (40.1 +/- 7.9) than before (44.4 +/- 7.6) the COVID-19 outbreak, we found that ICH was more likely to be observed by AI during than before the COVID-19 outbreak (p<0.05), with approximately one daily ICH+ case more than statistically expected. Conclusion: Our results suggest that, by tracking both large-scale utilization and AI results data in radiology, the tru-AI approach can contribute clinical value as a versatile exploratory tool, aiming at a better understanding of pandemic-related effects on healthcare.