 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeRT-Surv: Improving Mortality Prediction After Radiotherapy with Large Language Model Structuring of Large-Scale Unstructured Electronic Health Records
Aug 09, 2024Accurate patient selection is critical in radiotherapy (RT) to prevent ineffective treatments. Traditional survival prediction models, relying on structured data, often lack precision. This study explores the potential of large language models (LLMs) to structure unstructured electronic health record (EHR) data, thereby improving survival prediction accuracy through comprehensive clinical information integration. Data from 34,276 patients treated with RT at Yonsei Cancer Center between 2013 and 2023 were analyzed, encompassing both structured and unstructured data. An open-source LLM was used to structure the unstructured EHR data via single-shot learning, with its performance compared against a domain-specific medical LLM and a smaller variant. Survival prediction models were developed using statistical, machine learning, and deep learning approaches, incorporating both structured and LLM-structured data. Clinical experts evaluated the accuracy of the LLM-structured data. The open-source LLM achieved 87.5% accuracy in structuring unstructured EHR data without additional training, significantly outperforming the domain-specific medical LLM, which reached only 35.8% accuracy. Larger LLMs were more effective, particularly in extracting clinically relevant features like general condition and disease extent, which closely correlated with patient survival. Incorporating LLM-structured clinical features into survival prediction models significantly improved accuracy, with the C-index of deep learning models increasing from 0.737 to 0.820. These models also became more interpretable by emphasizing clinically significant factors. This study shows that general-domain LLMs, even without specific medical training, can effectively structure large-scale unstructured EHR data, substantially enhancing the accuracy and interpretability of clinical predictive models.
An Interpretable Web-based Glioblastoma Multiforme Prognosis Prediction Tool using Random Forest Model
Sep 09, 2021
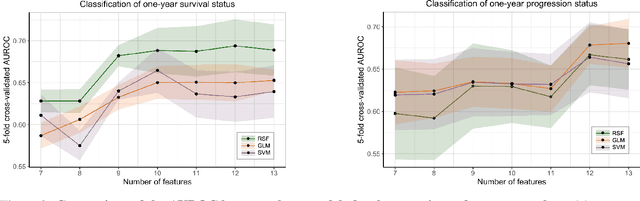
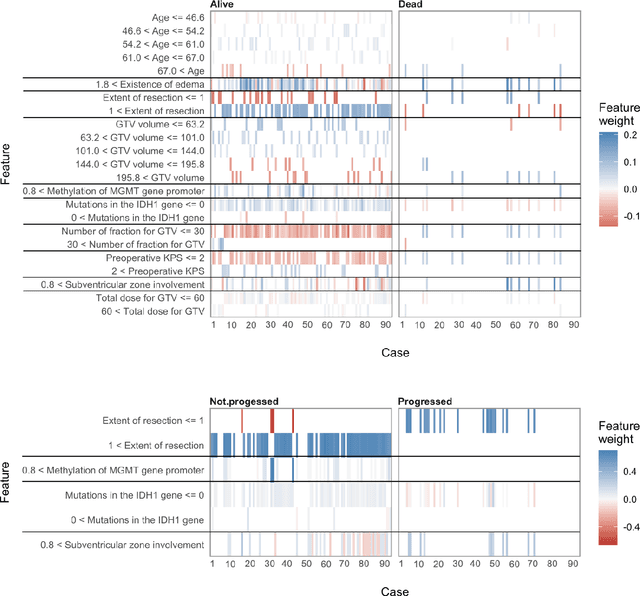

We propose predictive models that estimate GBM patients' health status of one-year after treatments (Classification task), predict the long-term prognosis of GBM patients at an individual level (Survival task). We used total of 467 GBM patients' clinical profile consists of 13 features and two follow-up dates. For baseline models of random forest classifier(RFC) and random survival forest model (RSF), we introduced generalized linear model (GLM), support vector machine (SVM) and Cox proportional hazardous model (COX), accelerated failure time model (AFT) respectively. After preprocessing and prefixing stratified 5-fold data set, we generated best performing models for model types using recursive feature elimination process. Total 10, 4, and 13 features were extracted for best performing one-year survival/progression status RFC models and RSF model via the recursive feature elimination process. In classification task, AUROC of best performing RFC recorded 0.6990 (for one-year survival status classification) and 0.7076 (for one-year progression classification) while that of second best baseline models (GLM in both cases) recorded 0.6691 and 0.6997 respectively. About survival task, the highest C-index of 0.7157 and the lowest IBS of 0.1038 came from the best performing RSF model while that of second best baseline models were 0.6556 and 0.1139 respectively. A simplified linear correlation (extracted from LIME and virtual patient group analysis) between each feature and prognosis of GBM patient were consistent with proven medical knowledge. Our machine learning models suggest that the top three prognostic factors for GBM patient survival were MGMT gene promoter, the extent of resection, and age. To the best of our knowledge, this study is the very first study introducing a interpretable and medical knowledge consistent GBM prognosis predictive models.