 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeBenchmarking the Impact of Noise on Deep Learning-based Classification of Atrial Fibrillation in 12-Lead ECG
Mar 24, 2023


Electrocardiography analysis is widely used in various clinical applications and Deep Learning models for classification tasks are currently in the focus of research. Due to their data-driven character, they bear the potential to handle signal noise efficiently, but its influence on the accuracy of these methods is still unclear. Therefore, we benchmark the influence of four types of noise on the accuracy of a Deep Learning-based method for atrial fibrillation detection in 12-lead electrocardiograms. We use a subset of a publicly available dataset (PTBXL) and use the metadata provided by human experts regarding noise for assigning a signal quality to each electrocardiogram. Furthermore, we compute a quantitative signal-to-noise ratio for each electrocardiogram. We analyze the accuracy of the Deep Learning model with respect to both metrics and observe that the method can robustly identify atrial fibrillation, even in cases signals are labelled by human experts as being noisy on multiple leads. False positive and false negative rates are slightly worse for data being labelled as noisy. Interestingly, data annotated as showing baseline drift noise results in an accuracy very similar to data without. We conclude that the issue of processing noisy electrocardiography data can be addressed successfully by Deep Learning methods that might not need preprocessing as many conventional methods do.
Analysis of a Deep Learning Model for 12-Lead ECG Classification Reveals Learned Features Similar to Diagnostic Criteria
Nov 03, 2022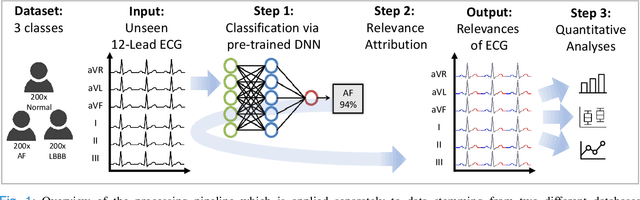
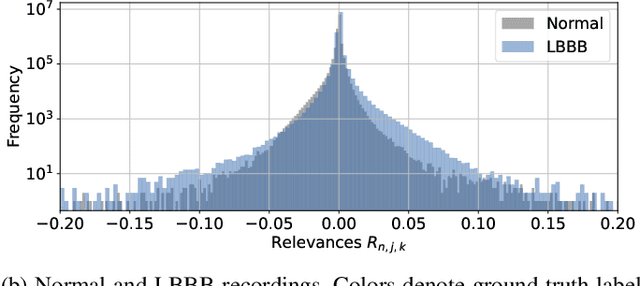

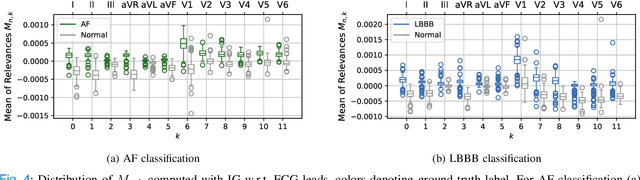
Despite their remarkable performance, deep neural networks remain unadopted in clinical practice, which is considered to be partially due to their lack in explainability. In this work, we apply attribution methods to a pre-trained deep neural network (DNN) for 12-lead electrocardiography classification to open this "black box" and understand the relationship between model prediction and learned features. We classify data from a public data set and the attribution methods assign a "relevance score" to each sample of the classified signals. This allows analyzing what the network learned during training, for which we propose quantitative methods: average relevance scores over a) classes, b) leads, and c) average beats. The analyses of relevance scores for atrial fibrillation (AF) and left bundle branch block (LBBB) compared to healthy controls show that their mean values a) increase with higher classification probability and correspond to false classifications when around zero, and b) correspond to clinical recommendations regarding which lead to consider. Furthermore, c) visible P-waves and concordant T-waves result in clearly negative relevance scores in AF and LBBB classification, respectively. In summary, our analysis suggests that the DNN learned features similar to cardiology textbook knowledge.