 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeAutomated Plaque Detection and Agatston Score Estimation on Non-Contrast CT Scans: A Multicenter Study
Feb 14, 2024Coronary artery calcification (CAC) is a strong and independent predictor of cardiovascular disease (CVD). However, manual assessment of CAC often requires radiological expertise, time, and invasive imaging techniques. The purpose of this multicenter study is to validate an automated cardiac plaque detection model using a 3D multiclass nnU-Net for gated and non-gated non-contrast chest CT volumes. CT scans were performed at three tertiary care hospitals and collected as three datasets, respectively. Heart, aorta, and lung segmentations were determined using TotalSegmentator, while plaques in the coronary arteries and heart valves were manually labeled for 801 volumes. In this work we demonstrate how the nnU-Net semantic segmentation pipeline may be adapted to detect plaques in the coronary arteries and valves. With a linear correction, nnU-Net deep learning methods may also accurately estimate Agatston scores on chest non-contrast CT scans. Compared to manual Agatson scoring, automated Agatston scoring indicated a slope of the linear regression of 0.841 with an intercept of +16 HU (R2 = 0.97). These results are an improvement over previous work assessing automated Agatston score computation in non-gated CT scans.
Automated Measurement of Pericoronary Adipose Tissue Attenuation and Volume in CT Angiography
Nov 22, 2023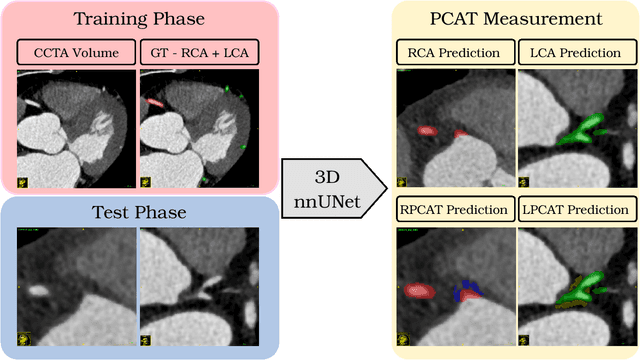
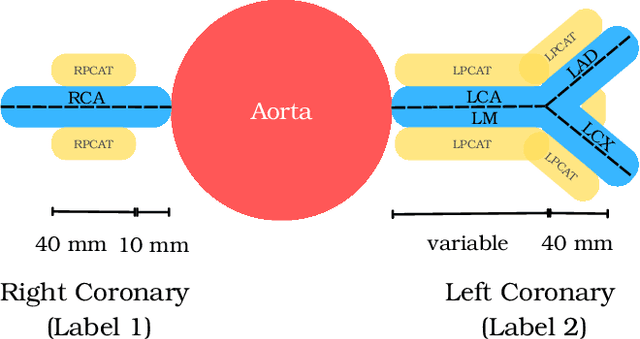


Pericoronary adipose tissue (PCAT) is the deposition of fat in the vicinity of the coronary arteries. It is an indicator of coronary inflammation and associated with coronary artery disease. Non-invasive coronary CT angiography (CCTA) is presently used to obtain measures of the thickness, volume, and attenuation of fat deposition. However, prior works solely focus on measuring PCAT using semi-automated approaches at the right coronary artery (RCA) over the left coronary artery (LCA). In this pilot work, we developed a fully automated approach for the measurement of PCAT mean attenuation and volume in the region around both coronary arteries. First, we used a large subset of patients from the public ImageCAS dataset (n = 735) to train a 3D full resolution nnUNet to segment LCA and RCA. Then, we automatically measured PCAT in the surrounding arterial regions. We evaluated our method on a held-out test set of patients (n = 183) from the same dataset. A mean Dice score of 83% and PCAT attenuation of -73.81 $\pm$ 12.69 HU was calculated for the RCA, while a mean Dice score of 81% and PCAT attenuation of -77.51 $\pm$ 7.94 HU was computed for the LCA. To the best of our knowledge, we are the first to develop a fully automated method to measure PCAT attenuation and volume at both the RCA and LCA. Our work underscores how automated PCAT measurement holds promise as a biomarker for identification of inflammation and cardiac disease.