 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeImproving ICD coding using Chapter based Named Entities and Attentional Models
Jul 24, 2024Recent advancements in natural language processing (NLP) have led to automation in various domains. However, clinical NLP often relies on benchmark datasets that may not reflect real-world scenarios accurately. Automatic ICD coding, a vital NLP task, typically uses outdated and imbalanced datasets like MIMIC-III, with existing methods yielding micro-averaged F1 scores between 0.4 and 0.7 due to many false positives. Our research introduces an enhanced approach to ICD coding that improves F1 scores by using chapter-based named entities and attentional models. This method categorizes discharge summaries into ICD-9 Chapters and develops attentional models with chapter-specific data, eliminating the need to consider external data for code identification. For categorization, we use Chapter-IV to de-bias and influence key entities and weights without neural networks, creating accurate thresholds and providing interpretability for human validation. Post-validation, we develop attentional models for three frequent and three non-frequent codes from Chapter-IV using Bidirectional-Gated Recurrent Units (GRUs) with Attention and Transformer with Multi-head Attention architectures. The average Micro-F1 scores of 0.79 and 0.81 from these models demonstrate significant performance improvements in ICD coding.
Methods to Measure the Broncho-Arterial Ratio and Wall Thickness in the Right Lower Lobe for Defining Radiographic Reversibility of Bronchiectasis
Jul 18, 2024


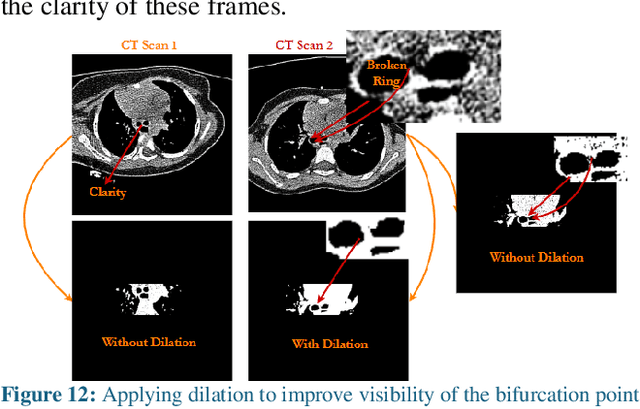
The diagnosis of bronchiectasis requires measuring abnormal bronchial dilation. It is confirmed using a chest CT scan, where the key feature is an increased broncho-arterial ratio (BAR) (>0.8 in children), often with bronchial wall thickening. Image processing methods facilitate quicker interpretation and detailed evaluations by lobes and segments. Challenges like inclined nature, oblique orientation, and partial volume effect make it difficult to obtain accurate measurements in the upper and middle lobes using the same algorithms. Therefore, accurate detection and measurement of airway and artery regions for BAR and wall thickness in each lobe require different image processing/machine learning methods. We propose methods for: 1. Separating the right lower lobe (RLL) region from full-length CT scans using the tracheal bifurcation (Carina) point as a central marker; 2. Locating the inner diameter of airways and outer diameter of arteries for BAR measurement; and 3. Measuring airway wall thickness (WT) by identifying the outer and inner diameters of airway boundaries. Analysis of 13 HRCT scans with varying thicknesses (0.67mm, 1mm, 2mm) shows the tracheal bifurcation frame can be detected accurately, with a deviation of +/- 2 frames in some cases. A Windows app was developed for measuring inner airway diameter, artery diameter, BAR, and wall thickness, allowing users to draw boundaries around visible BA pairs in the RLL region. Measurements of 10 BA pairs revealed accurate results comparable to those of a human reader, with deviations of +/- 0.10-0.15mm. Additional studies and validation are needed to consolidate inter- and intra-rater variability and enhance the methods.