 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeShape Analysis for Pediatric Upper Body Motor Function Assessment
Paper and Code
Sep 10, 2022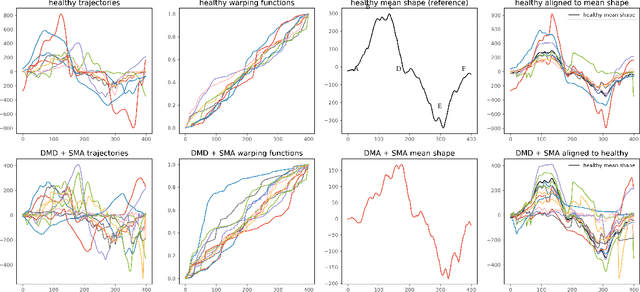



Neuromuscular disorders, such as Spinal Muscular Atrophy (SMA) and Duchenne Muscular Dystrophy (DMD), cause progressive muscular degeneration and loss of motor function for 1 in 6,000 children. Traditional upper limb motor function assessments do not quantitatively measure patient-performed motions, which makes it difficult to track progress for incremental changes. Assessing motor function in children with neuromuscular disorders is particularly challenging because they can be nervous or excited during experiments, or simply be too young to follow precise instructions. These challenges translate to confounding factors such as performing different parts of the arm curl slower or faster (phase variability) which affects the assessed motion quality. This paper uses curve registration and shape analysis to temporally align trajectories while simultaneously extracting a mean reference shape. Distances from this mean shape are used to assess the quality of motion. The proposed metric is invariant to confounding factors, such as phase variability, while suggesting several clinically relevant insights. First, there are statistically significant differences between functional scores for the control and patient populations (p$=$0.0213$\le$0.05). Next, several patients in the patient cohort are able to perform motion on par with the healthy cohort and vice versa. Our metric, which is computed based on wearables, is related to the Brooke's score ((p$=$0.00063$\le$0.05)), as well as motor function assessments based on dynamometry ((p$=$0.0006$\le$0.05)). These results show promise towards ubiquitous motion quality assessment in daily life.