 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgePredicting adverse outcomes following catheter ablation treatment for atrial fibrillation
Paper and Code
Nov 22, 2022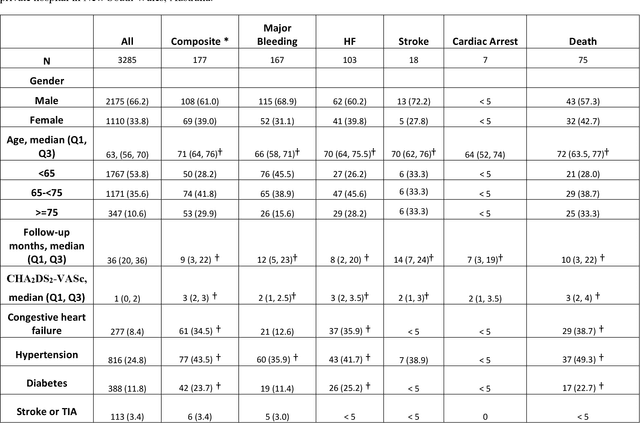
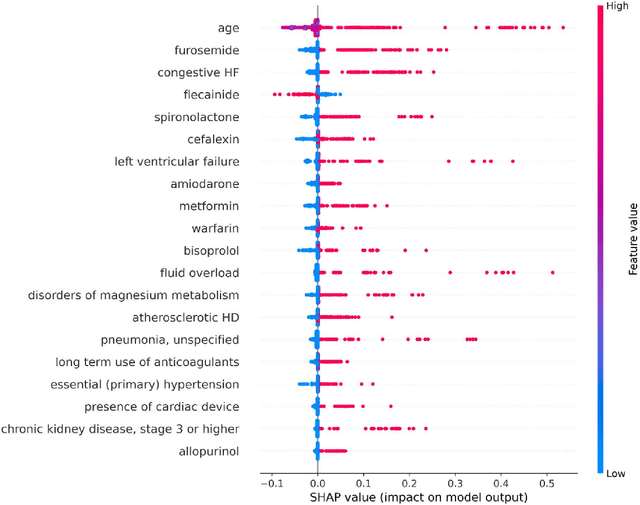
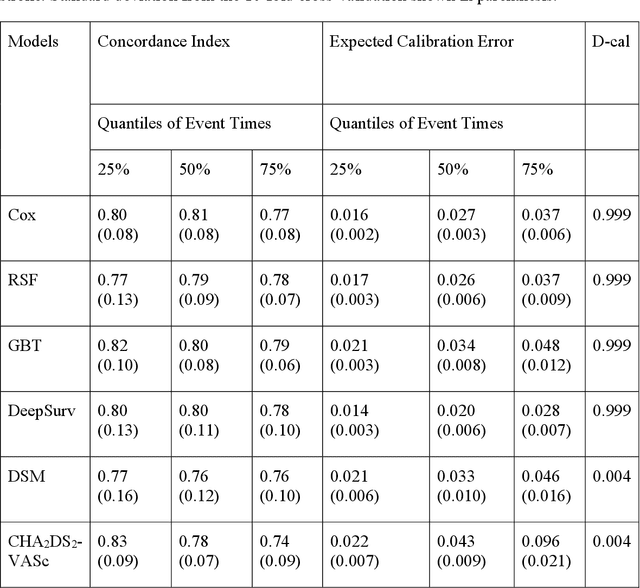
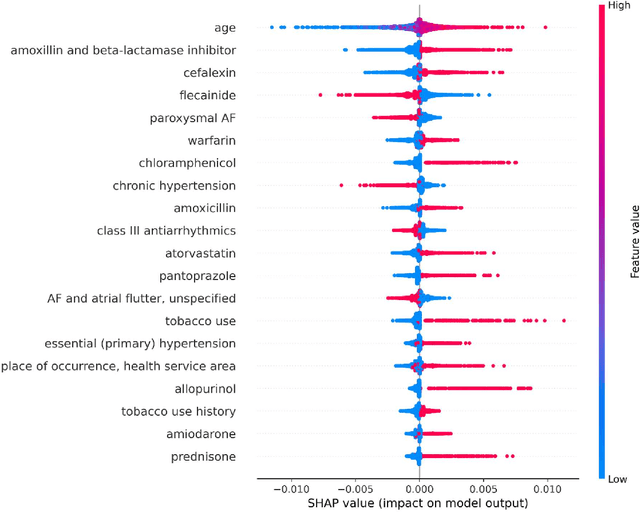
Objective: To develop prognostic survival models for predicting adverse outcomes after catheter ablation treatment for non-valvular atrial fibrillation (AF). Methods: We used a linked dataset including hospital administrative data, prescription medicine claims, emergency department presentations, and death registrations of patients in New South Wales, Australia. The cohort included patients who received catheter ablation for AF. Traditional and deep survival models were trained to predict major bleeding events and a composite of heart failure, stroke, cardiac arrest, and death. Results: Out of a total of 3285 patients in the cohort, 177 (5.3%) experienced the composite outcomeheart failure, stroke, cardiac arrest, deathand 167 (5.1%) experienced major bleeding events after catheter ablation treatment. Models predicting the composite outcome had high risk discrimination accuracy, with the best model having a concordance index > 0.79 at the evaluated time horizons. Models for predicting major bleeding events had poor risk discrimination performance, with all models having a concordance index < 0.66. The most impactful features for the models predicting higher risk were comorbidities indicative of poor health, older age, and therapies commonly used in sicker patients to treat heart failure and AF. Conclusions: Diagnosis and medication history did not contain sufficient information for precise risk prediction of experiencing major bleeding events. The models for predicting the composite outcome have the potential to enable clinicians to identify and manage high-risk patients following catheter ablation proactively. Future research is needed to validate the usefulness of these models in clinical practice.