 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeAutomated Pain Detection from Facial Expressions using FACS: A Review
Nov 13, 2018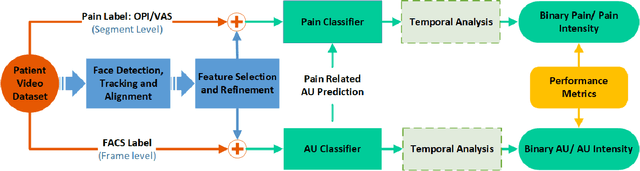
Facial pain expression is an important modality for assessing pain, especially when the patient's verbal ability to communicate is impaired. The facial muscle-based action units (AUs), which are defined by the Facial Action Coding System (FACS), have been widely studied and are highly reliable as a method for detecting facial expressions (FE) including valid detection of pain. Unfortunately, FACS coding by humans is a very time-consuming task that makes its clinical use prohibitive. Significant progress on automated facial expression recognition (AFER) has led to its numerous successful applications in FACS-based affective computing problems. However, only a handful of studies have been reported on automated pain detection (APD), and its application in clinical settings is still far from a reality. In this paper, we review the progress in research that has contributed to automated pain detection, with focus on 1) the framework-level similarity between spontaneous AFER and APD problems; 2) the evolution of system design including the recent development of deep learning methods; 3) the strategies and considerations in developing a FACS-based pain detection framework from existing research; and 4) introduction of the most relevant databases that are available for AFER and APD studies. We attempt to present key considerations in extending a general AFER framework to an APD framework in clinical settings. In addition, the performance metrics are also highlighted in evaluating an AFER or an APD system.
Learning Pain from Action Unit Combinations: A Weakly Supervised Approach via Multiple Instance Learning
Feb 20, 2018



Patient pain can be detected highly reliably from facial expressions using a set of facial muscle-based action units (AUs) defined by the Facial Action Coding System (FACS). A key characteristic of facial expression of pain is the simultaneous occurrence of pain-related AU combinations, whose automated detection would be highly beneficial for efficient and practical pain monitoring. Existing general Automated Facial Expression Recognition (AFER) systems prove inadequate when applied specifically for detecting pain as they either focus on detecting individual pain-related AUs but not on combinations or they seek to bypass AU detection by training a binary pain classifier directly on pain intensity data but are limited by lack of enough labeled data for satisfactory training. In this paper, we propose a new approach that mimics the strategy of human coders of decoupling pain detection into two consecutive tasks: one performed at the individual video-frame level and the other at video-sequence level. Using state-of-the-art AFER tools to detect single AUs at the frame level, we propose two novel data structures to encode AU combinations from single AU scores. Two weakly supervised learning frameworks namely multiple instance learning (MIL) and multiple clustered instance learning (MCIL) are employed corresponding to each data structure to learn pain from video sequences. Experimental results show an 87% pain recognition accuracy with 0.94 AUC (Area Under Curve) on the UNBC-McMaster Shoulder Pain Expression dataset. Tests on long videos in a lung cancer patient video dataset demonstrates the potential value of the proposed system for pain monitoring in clinical settings.