 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgePerformance of multilabel machine learning models and risk stratification schemas for predicting stroke and bleeding risk in patients with non-valvular atrial fibrillation
Feb 02, 2022
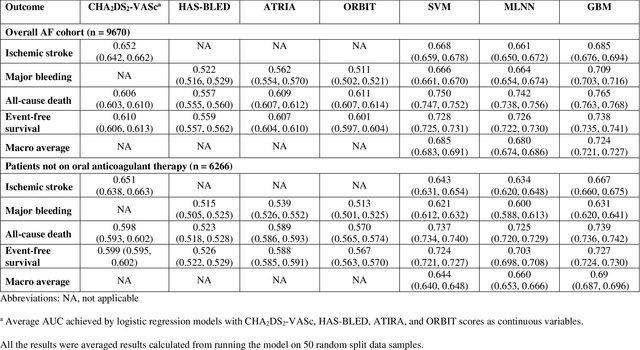
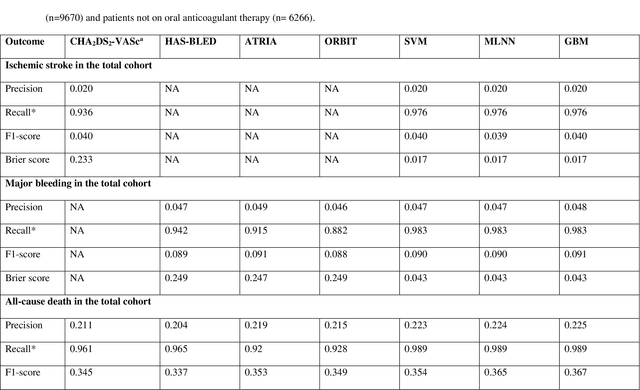
Appropriate antithrombotic therapy for patients with atrial fibrillation (AF) requires assessment of ischemic stroke and bleeding risks. However, risk stratification schemas such as CHA2DS2-VASc and HAS-BLED have modest predictive capacity for patients with AF. Machine learning (ML) techniques may improve predictive performance and support decision-making for appropriate antithrombotic therapy. We compared the performance of multilabel ML models with the currently used risk scores for predicting outcomes in AF patients. Materials and Methods This was a retrospective cohort study of 9670 patients, mean age 76.9 years, 46% women, who were hospitalized with non-valvular AF, and had 1-year follow-up. The primary outcome was ischemic stroke and major bleeding admission. The secondary outcomes were all-cause death and event-free survival. The discriminant power of ML models was compared with clinical risk scores by the area under the curve (AUC). Risk stratification was assessed using the net reclassification index. Results Multilabel gradient boosting machine provided the best discriminant power for stroke, major bleeding, and death (AUC = 0.685, 0.709, and 0.765 respectively) compared to other ML models. It provided modest performance improvement for stroke compared to CHA2DS2-VASc (AUC = 0.652), but significantly improved major bleeding prediction compared to HAS-BLED (AUC = 0.522). It also had a much greater discriminant power for death compared with CHA2DS2-VASc (AUC = 0.606). Also, models identified additional risk features (such as hemoglobin level, renal function, etc.) for each outcome. Conclusions Multilabel ML models can outperform clinical risk stratification scores for predicting the risk of major bleeding and death in non-valvular AF patients.