 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeUndersampling and Bagging of Decision Trees in the Analysis of Cardiorespiratory Behavior for the Prediction of Extubation Readiness in Extremely Preterm Infants
Aug 24, 2018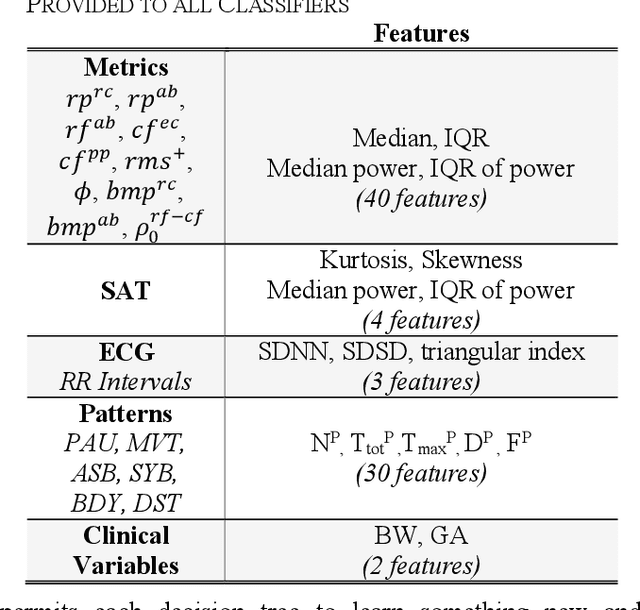
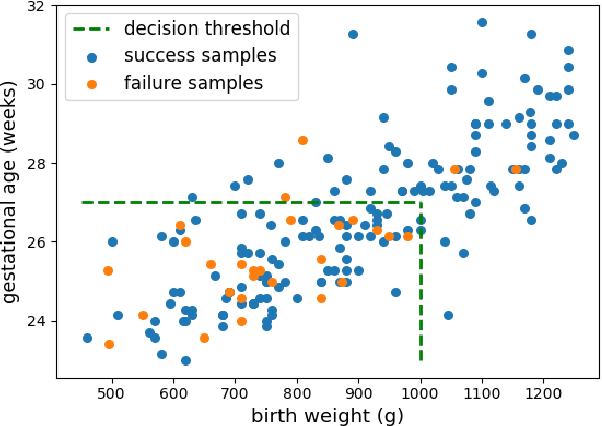

Extremely preterm infants often require endotracheal intubation and mechanical ventilation during the first days of life. Due to the detrimental effects of prolonged invasive mechanical ventilation (IMV), clinicians aim to extubate infants as soon as they deem them ready. Unfortunately, existing strategies for prediction of extubation readiness vary across clinicians and institutions, and lead to high reintubation rates. We present an approach using Random Forest classifiers for the analysis of cardiorespiratory variability to predict extubation readiness. We address the issue of data imbalance by employing random undersampling of examples from the majority class before training each Decision Tree in a bag. By incorporating clinical domain knowledge, we further demonstrate that our classifier could have identified 71% of infants who failed extubation, while maintaining a success detection rate of 78%.
Predicting Extubation Readiness in Extreme Preterm Infants based on Patterns of Breathing
Aug 24, 2018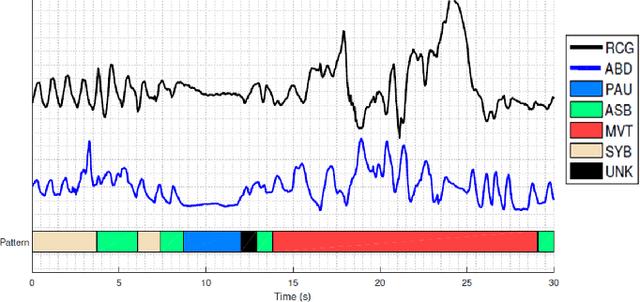

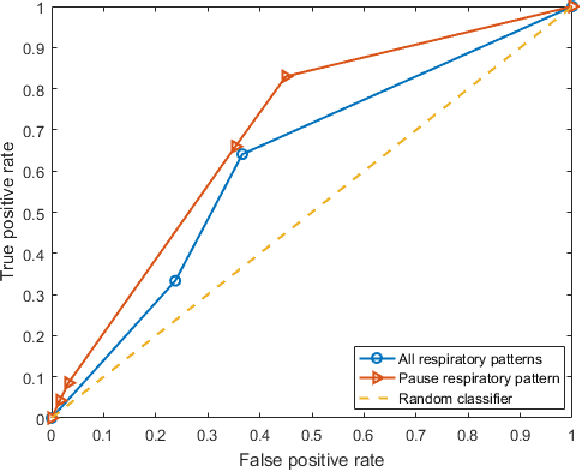

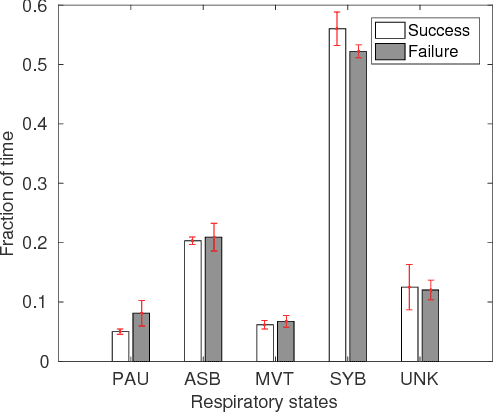
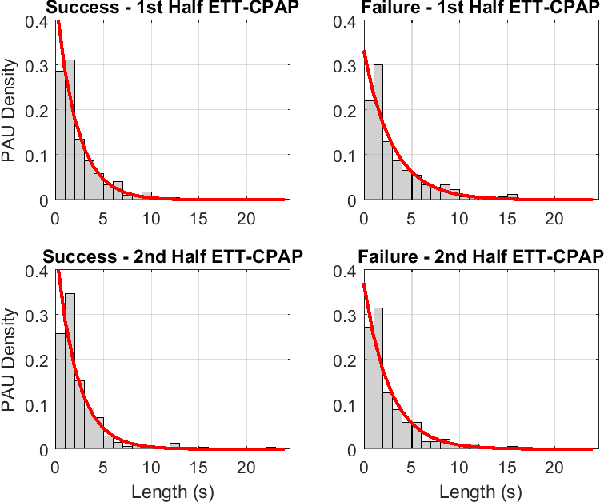
Extremely preterm infants commonly require intubation and invasive mechanical ventilation after birth. While the duration of mechanical ventilation should be minimized in order to avoid complications, extubation failure is associated with increases in morbidities and mortality. As part of a prospective observational study aimed at developing an accurate predictor of extubation readiness, Markov and semi-Markov chain models were applied to gain insight into the respiratory patterns of these infants, with more robust time-series modeling using semi-Markov models. This model revealed interesting similarities and differences between newborns who succeeded extubation and those who failed. The parameters of the model were further applied to predict extubation readiness via generative (joint likelihood) and discriminative (support vector machine) approaches. Results showed that up to 84\% of infants who failed extubation could have been accurately identified prior to extubation.
A Semi-Markov Chain Approach to Modeling Respiratory Patterns Prior to Extubation in Preterm Infants
Aug 24, 2018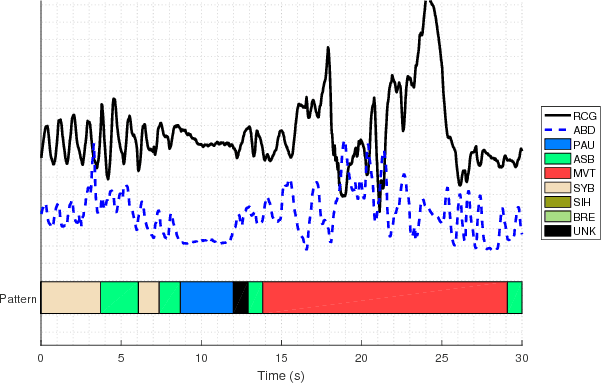
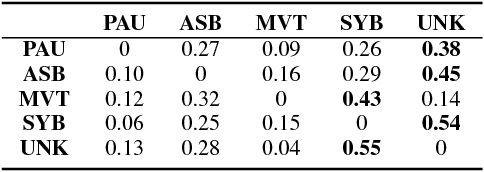
After birth, extremely preterm infants often require specialized respiratory management in the form of invasive mechanical ventilation (IMV). Protracted IMV is associated with detrimental outcomes and morbidities. Premature extubation, on the other hand, would necessitate reintubation which is risky, technically challenging and could further lead to lung injury or disease. We present an approach to modeling respiratory patterns of infants who succeeded extubation and those who required reintubation which relies on Markov models. We compare the use of traditional Markov chains to semi-Markov models which emphasize cross-pattern transitions and timing information, and to multi-chain Markov models which can concisely represent non-stationarity in respiratory behavior over time. The models we developed expose specific, unique similarities as well as vital differences between the two populations.