 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeUndersampling and Bagging of Decision Trees in the Analysis of Cardiorespiratory Behavior for the Prediction of Extubation Readiness in Extremely Preterm Infants
Paper and Code
Aug 24, 2018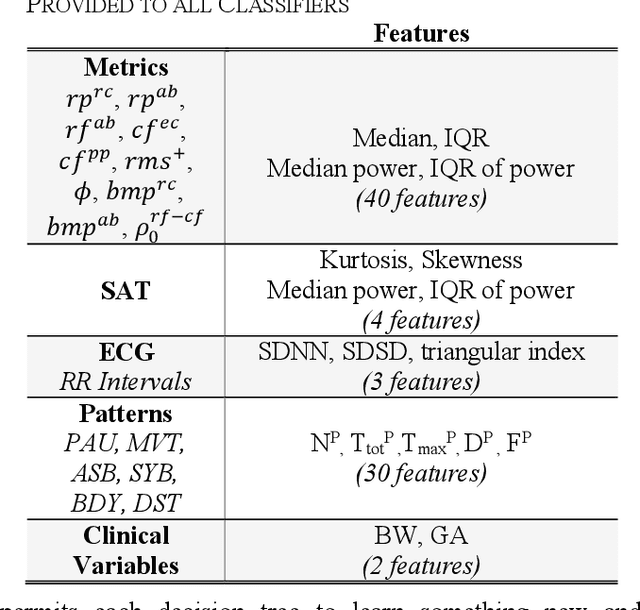
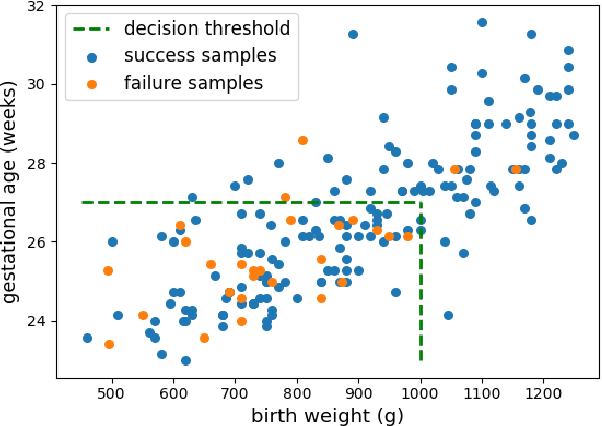

Extremely preterm infants often require endotracheal intubation and mechanical ventilation during the first days of life. Due to the detrimental effects of prolonged invasive mechanical ventilation (IMV), clinicians aim to extubate infants as soon as they deem them ready. Unfortunately, existing strategies for prediction of extubation readiness vary across clinicians and institutions, and lead to high reintubation rates. We present an approach using Random Forest classifiers for the analysis of cardiorespiratory variability to predict extubation readiness. We address the issue of data imbalance by employing random undersampling of examples from the majority class before training each Decision Tree in a bag. By incorporating clinical domain knowledge, we further demonstrate that our classifier could have identified 71% of infants who failed extubation, while maintaining a success detection rate of 78%.