 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeImplementation and Evaluation of a System for Assessment of The Quality of Long-Term Management of Patients at a Geriatric Hospital
Nov 23, 2022



Background The use of a clinical decision support system for assessing the quality of care, based on computerized clinical guidelines (GLs), is likely to improve care, reduce costs, save time, and enhance the staff's capabilities. Objectives Implement and evaluate a system for assessment of the quality of the care, in the domain of management of pressure ulcers, by investigating the level of compliance of the staff to the GLs. Methods Using data for 100 random patients from the local EMR system we performed a technical evaluation, checking the applicability and usability, followed by a functional evaluation of the system investigating the quality metrics given to the compliance of the medical's staff to the protocol. We compared the scores given by the nurse when supported by the system, to the scores given by the nurse without the system's support, and to the scores given by the system. We also measured the time taken to perform the assessment with and without the system's support. Results There were no significant differences in the scores of most measures given by the nurse using the system, compared to the scores given by the system. There were also no significant differences across the values of most quality measures given by the nurse without support compared to the values given by the nurse with support. Using the system, however, significantly reduced the nurse's average assessment time. Conclusions Using an automated quality-assessment system, may enable a senior nurse, to quickly and accurately assess the quality of care. In addition to its accuracy, the system considerably reduces the time taken to assess the various quality measures.
Distributed Application of Guideline-Based Decision Support through Mobile Devices: Implementation and Evaluation
Feb 22, 2021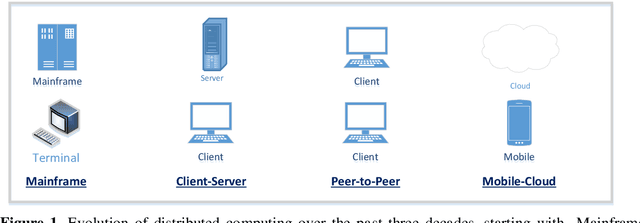

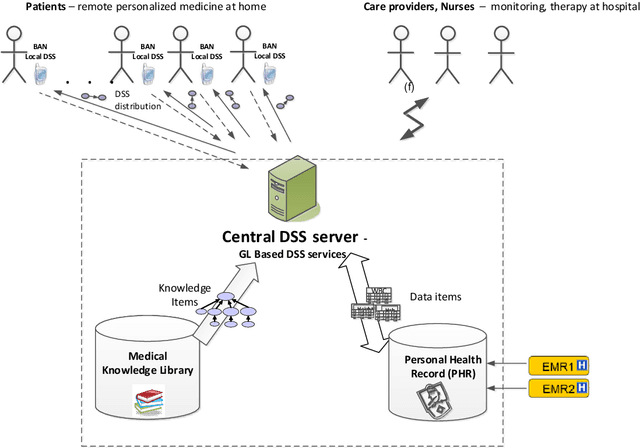
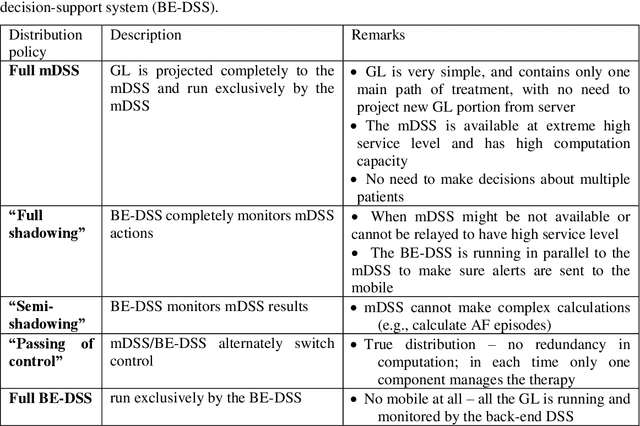
Traditionally Guideline(GL)based Decision Support Systems (DSSs) use a centralized infrastructure to generate recommendations to care providers. However, managing patients at home is preferable, reducing costs and empowering patients. We aimed to design, implement, and demonstrate the feasibility of a new architecture for a distributed DSS that provides patients with personalized, context-sensitive, evidence based guidance through their mobile device, and increases the robustness of the distributed application of the GL, while maintaining access to the patient longitudinal record and to an up to date evidence based GL repository. We have designed and implemented a novel projection and callback (PCB) model, in which small portions of the evidence based GL procedural knowledge, adapted to the patient preferences and to their current context, are projected from a central DSS server, to a local DSS on the patient mobile device that applies that knowledge. When appropriate, as defined by a temporal pattern within the projected plan, the local DSS calls back the central DSS, requesting further assistance, possibly another projection. Thus, the GL specification includes two levels: one for the central DSS, one for the local DSS. We successfully evaluated the PCB model within the MobiGuide EU project by managing Gestational Diabetes Mellitus patients in Spain, and Atrial Fibrillation patients in Italy. Significant differences exist between the two GL representations, suggesting additional ways to characterize GLs. Mean time between the central and local interactions was quite different for the two GLs: 3.95 days for gestational diabetes, 23.80 days for atrial fibrillation. Most interactions, 83%, were due to projections to the mDSS. Others were data notifications, mostly to change context. Robustness was demonstrated through successful recovery from multiple local DSS crashes.