 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeBayesian Meta-Analyses Could Be More: A Case Study in Trial of Labor After a Cesarean-section Outcomes and Complications
Jan 15, 2026The meta-analysis's utility is dependent on previous studies having accurately captured the variables of interest, but in medical studies, a key decision variable that impacts a physician's decisions was not captured. This results in an unknown effect size and unreliable conclusions. A Bayesian approach may allow analysis to determine if the claim of a positive effect is still warranted, and we build a Bayesian approach to this common medical scenario. To demonstrate its utility, we assist professional OBGYNs in evaluating Trial of Labor After a Cesarean-section (TOLAC) situations where few interventions are available for patients and find the support needed for physicians to advance patient care.
More Options for Prelabor Rupture of Membranes, A Bayesian Analysis
Aug 20, 2024


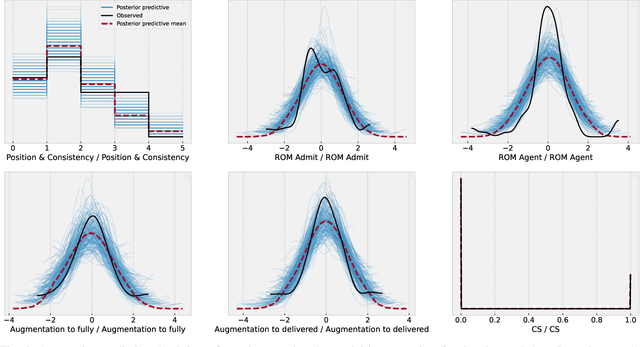
An obstetric goal for a laboring mother is to achieve a vaginal delivery as it reduces the risks inherent in major abdominal surgery (i.e., a Cesarean section). Various medical interventions may be used by a physician to increase the likelihood of this occurring while minimizing maternal and fetal morbidity. However, patients with prelabor rupture of membranes (PROM) have only two commonly used options for cervical ripening, Pitocin and misoprostol. Little research exists on the benefits/risks for these two key drugs for PROM patients. A major limitation with most induction-of-labor related research is the inability to account for differences in \textit{Bishop scores} that are commonly used in obstetrical practice to determine the next induction agent offered to the patient. This creates a confounding factor, which biases the results, but has not been realized in the literature. In this work, we use a Bayesian model of the relationships between the relevant factors, informed by expert physicians, to separate the confounding variable from its actual impact. In doing so, we provide strong evidence that pitocin and buccal misoprostol are equally effective and safe; thus, physicians have more choice in clinical care than previously realized. This is particularly important for developing countries where neither medication may be readily available, and prior guidelines may create an artificial barrier to needed medication.