 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeOptimal Sensor Placement in Body Surface Networks using Gaussian Processes
Sep 07, 2022


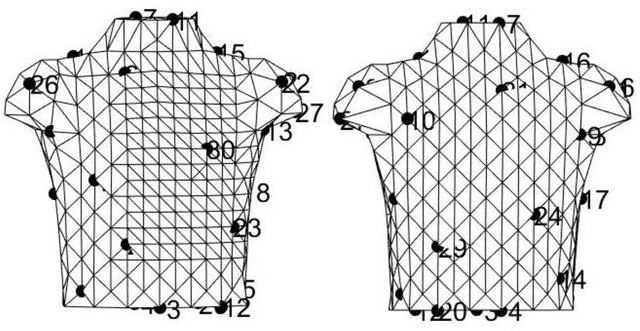
This paper explores a new sequential selection framework for the optimal sensor placement (OSP) in Electrocardiography imaging networks (ECGI). The proposed methodology incorporates the use a recent experimental design method for the sequential selection of landmarkings on biological objects, namely, Gaussian process landmarking (GPLMK) for better exploration of the candidate sensors. The two experimental design methods work as a source of the training and the validation locations which is fitted using a spatiotemporal Gaussian process (STGP). The STGP is fitted using the training set to predict for the current validation set generated using GPLMK, and the sensor with the largest prediction absolute error is selected from the current validation set and added to the selected sensors. Next, a new validation set is generated and predicted using the current training set. The process continues until selecting a specific number of sensor locations. The study is conducted on a dataset of body surface potential mapping (BSPM) of 352 electrodes of four human subjects. A number of 30 sensor locations is selected using the proposed algorithm. The selected sensor locations achieved average $R^2 = 94.40 \%$ for estimating the whole-body QRS segment. The proposed method adds to design efforts for a more clinically practical ECGI system by improving its wearability and reduce the design cost as well.
Modeling patient flow in the emergency department using machine learning and simulation
Nov 22, 2020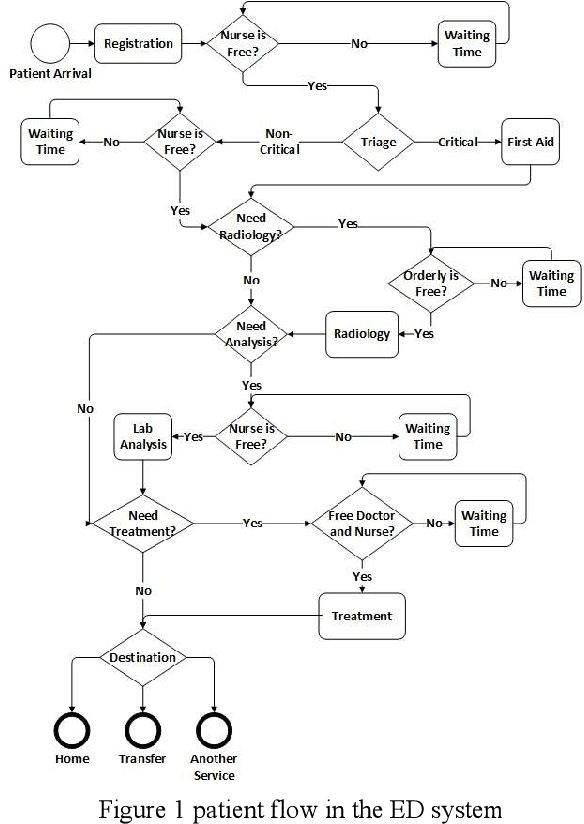
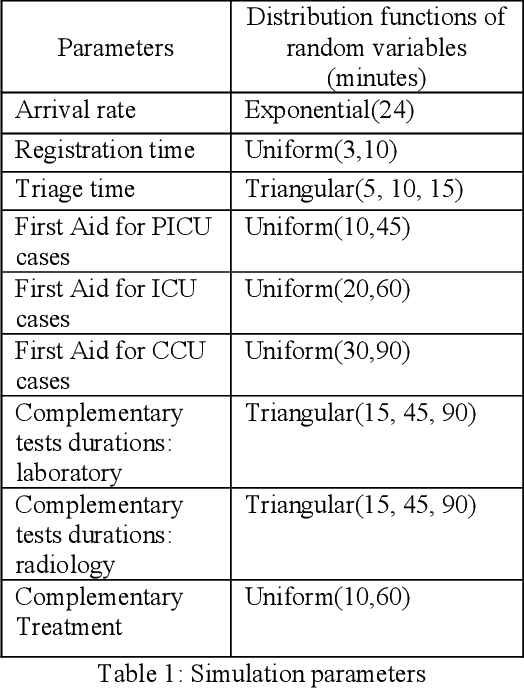
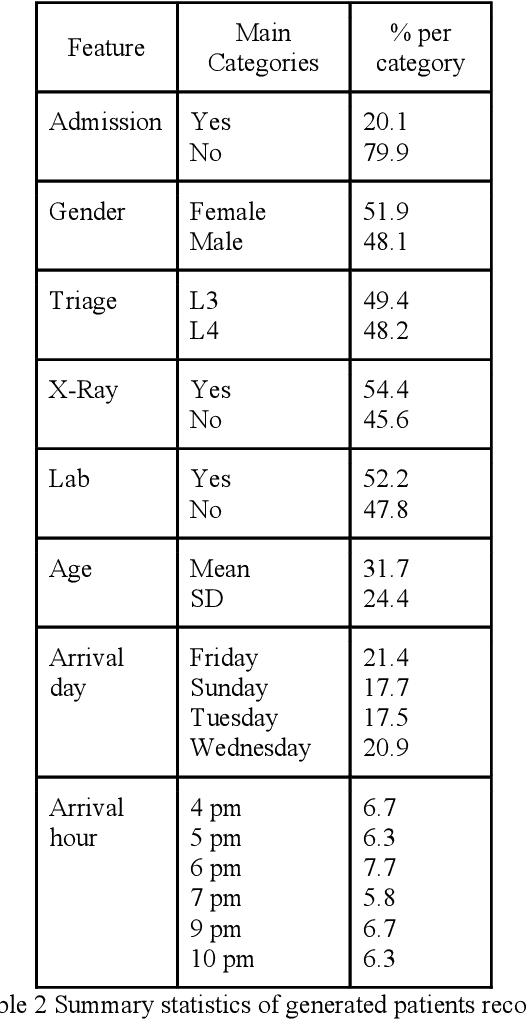
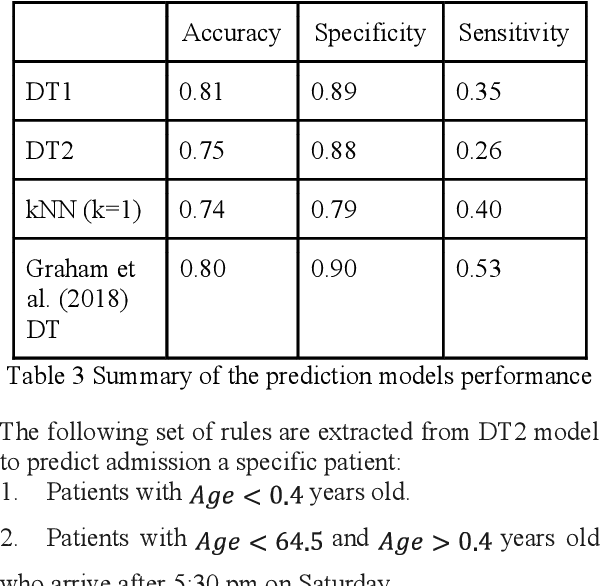
Recently, the combination of machine learning (ML) and simulation is gaining a lot of attention. This paper presents a novel application of ML within the simulation to improve patient flow within an emergency department (ED). An ML model used within a real ED simulation model to quantify the effect of detouring a patient out of the ED on the length of stay (LOS) and door-to-doctor time (DTDT) as a response to the prediction of patient admission to the hospital from the ED. The ML model trained using a set of six features including the patient age, arrival day, arrival hour of the day, and the triage level. The prediction model used a decision tree (DT) model, which is trained using historical data achieves a 75% accuracy. The set of rules extracted from the DT are coded within the simulation model. Given a certain probability of free inpatient beds, the predicted admitted patient is then pulled out from the ED to inpatient units to alleviate the crowding within the ED. The used policy combined with adding specific ED resources achieve 9.39% and 8.18% reduction in LOS and DTDT, respectively.