 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeODEWS: The Overdraft Early Warning System
Feb 05, 2023When a customer overdraws their account and their balance is negative they are assessed an overdraft fee. Americans pay approximately \$15 billion in unnecessary overdraft fees a year, often in \$35 increments; users of the Mint personal finance app pay approximately \$250 million in fees a year in particular. These overdraft fees are an excessive financial burden and lead to cascading overdraft fees trapping customers in financial hardship. To address this problem, we have created an ML-driven overdraft early warning system (ODEWS) that assesses a customer's risk of overdrafting within the next week using their banking and transaction data in the Mint app. At-risk customers are sent an alert so they can take steps to avoid the fee, ultimately changing their behavior and financial habits. The system deployed resulted in a \$3 million savings in overdraft fees for Mint customers compared to a control group. Moreover, the methodology outlined here can be generalized to provide ML-driven personalized financial advice for many different personal finance goals--increase credit score, build emergency savings fund, pay down debut, allocate capital for investment.
A Machine Learning System for Retaining Patients in HIV Care
Jun 01, 2020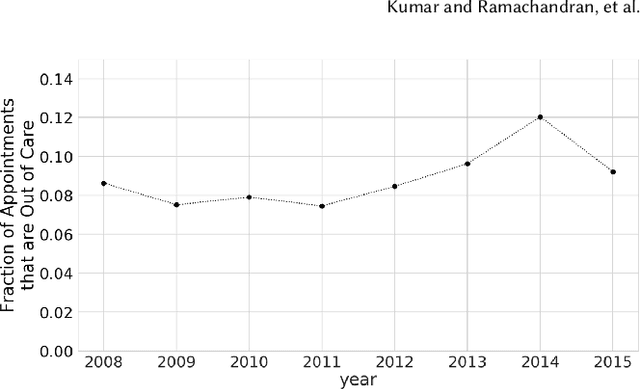
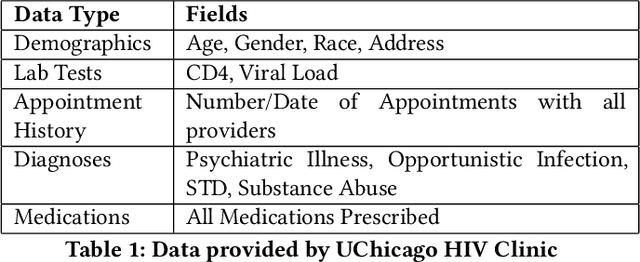
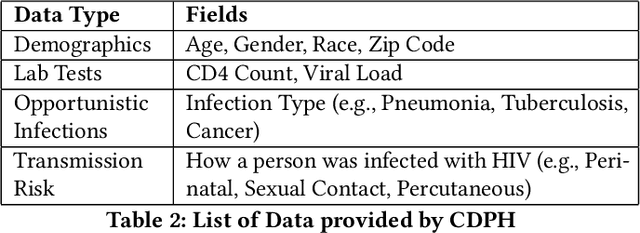
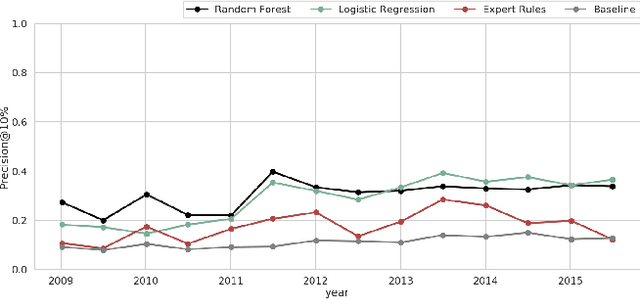
Retaining persons living with HIV (PLWH) in medical care is paramount to preventing new transmissions of the virus and allowing PLWH to live normal and healthy lifespans. Maintaining regular appointments with an HIV provider and taking medication daily for a lifetime is exceedingly difficult. 51% of PLWH are non-adherent with their medications and eventually drop out of medical care. Current methods of re-linking individuals to care are reactive (after a patient has dropped-out) and hence not very effective. We describe our system to predict who is most at risk to drop-out-of-care for use by the University of Chicago HIV clinic and the Chicago Department of Public Health. Models were selected based on their predictive performance under resource constraints, stability over time, as well as fairness. Our system is applicable as a point-of-care system in a clinical setting as well as a batch prediction system to support regular interventions at the city level. Our model performs 3x better than the baseline for the clinical model and 2.3x better than baseline for the city-wide model. The code has been released on github and we hope this methodology, particularly our focus on fairness, will be adopted by other clinics and public health agencies in order to curb the HIV epidemic.